Large Vessel Occlusion Strokes
Prehospital Stroke Severity Scales
Rapid identification of patients with a large vessel occlusion (LVO) is one of the most important decisions EMS providers make in the care of an acute stroke patient. While all suspected stroke patients require rapid transport, those with an LVO may benefit from mechanical thrombectomy, a time-sensitive procedure that is available only at Comprehensive Stroke Centers such as the University of Iowa. Because of this, EMS providers use validated stroke severity scales to identify patients who are at high risk for LVO and determine the most appropriate destination hospital. Several prehospital stroke severity tools have been developed to assist with this decision, but the most commonly referenced in EMS practice are the RACE, LAMS, VAN, CPSSS, and FAST-ED scales. Although each has demonstrated value in identifying potential LVOs, they differ in complexity, the neurological deficits they evaluate, and their overall diagnostic performance.
RACE (Rapid Arterial Occlusion Evaluation)
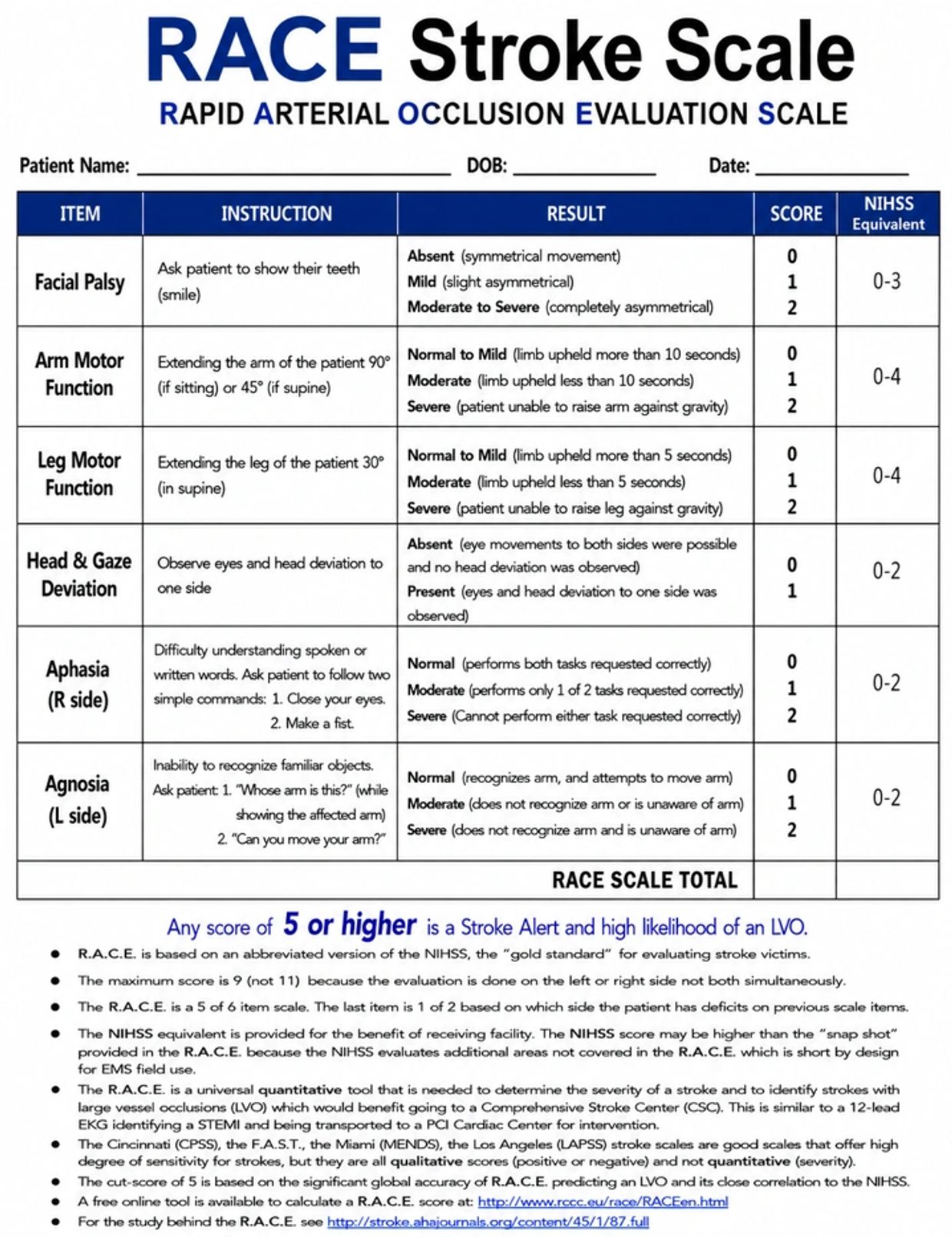
The RACE scale evaluates facial palsy, arm and leg motor function, head and gaze deviation, and cortical signs such as aphasia or agnosia to identify patients with suspected large vessel occlusion (LVO). It provides a quantitative score from 0–9, allowing EMS providers to estimate stroke severity while identifying patients most likely to benefit from mechanical thrombectomy.
LAMS (Los Angeles Motor Scale)
The LAMS evaluates facial droop, arm drift, and grip strength to estimate stroke severity. While it is quick and easy to perform, it relies almost entirely on motor deficits and does not assess important cortical findings like gaze deviation, aphasia, or neglect, making it less accurate for identifying LVOs.
VAN (Vision, Aphasia, Neglect)
The VAN assessment first identifies arm weakness and then looks for cortical signs including vision changes, aphasia, and neglect. It is a simple positive-or-negative screening tool designed to rapidly identify patients who may have an LVO but does not quantify stroke severity.
CPSSS (Cincinnati Prehospital Stroke Severity Scale)
The CPSSS is an extension of the Cincinnati Prehospital Stroke Scale that was developed to help EMS providers rapidly identify patients at high risk for a large vessel occlusion (LVO). It evaluates conjugate gaze deviation, severe arm weakness, and abnormalities in level of consciousness, producing a score from 0–4.
FAST-ED (Field Assessment Stroke Triage for Emergency Destination)
The FAST-ED scale builds upon the traditional FAST assessment by adding eye deviation and cortical deficits such as aphasia and neglect. It provides a severity score and has good diagnostic accuracy for LVO, but it requires more detailed neurological assessment and is somewhat more complex to perform in the prehospital setting.
Why the RACE Scale is Preferred for EMS
Among the available prehospital stroke severity tools, the RACE (Rapid Arterial Occlusion Evaluation) scale provides a combination of simplicity, speed, and diagnostic accuracy for identifying patients with a suspected large vessel occlusion (LVO). Unlike LAMS, RACE evaluates important cortical findings, including gaze deviation, aphasia, and neglect, which are among the strongest clinical predictors of an LVO. Unlike VAN, which was designed as a secondary assessment to be performed only after a patient has already screened positive for stroke and demonstrated arm weakness, the RACE scale is a standalone tool that simultaneously identifies stroke, quantifies its severity, and estimates the likelihood of an LVO, eliminating the need for multiple sequential assessments. While CPSSS is also a rapid and effective screening tool, it evaluates only gaze deviation, arm weakness, and level of consciousness, omitting leg weakness and several cortical deficits that improve LVO detection. FAST-ED has diagnostic performance comparable to RACE, but it requires a more detailed neurological examination and is somewhat more complex to perform in the prehospital setting. The RACE scale was specifically developed for EMS providers and has been extensively validated in the field, demonstrating approximately 85% sensitivity and 68% specificity for detecting LVO when a score of 5 or greater is used. Its ease of use, comprehensive neurological assessment, quantitative scoring system, strong predictive performance, and ability to guide destination decisions for transport to a Comprehensive Stroke Center make the RACE scale a practical and effective LVO screening tool.
RACE Stroke Assessment